For primary tauopathies, donated brain tissue and fluids are more than biological materials. They are the raw evidence scientists need to build earlier diagnostics, measure disease progression, and test new treatments. Click to download our most recent report.
Imagine trying to solve a medical mystery with only a few pages of the case file. That is the challenge many researchers are facing as they work on primary tauopathies, a group of neurodegenerative diseases in which abnormal tau protein builds up in the brain and contributes to the loss of brain cells. These diseases include progressive supranuclear palsy (PSP), corticobasal degeneration (CBD), Pick’s disease, argyrophilic grain disease, chronic traumatic encephalopathy (CTE), and related conditions. They can affect movement, thinking, behavior, language, balance, and independence, but the early symptoms often overlap with other neurologic diseases.
Today, many people with a suspected primary tauopathy are diagnosed based on symptoms, neurologic examination, brain imaging, and clinical judgment. That approach is valuable, but it is imperfect. PSP can resemble Parkinson’s disease. Corticobasal syndrome can be caused by CBD, PSP, Alzheimer’s disease (AD), or other pathologies. Some frontotemporal dementia syndromes can be driven by tau, while others are driven by different proteins. In most cases, the most definitive diagnosis still comes from examining brain tissue after death.
This is why biomarkers matter. A biomarker is a measurable biological clue that helps detect a disease, estimate its stage, or track how it changes over time (e.g., a protein pattern in blood or cerebrospinal fluid (CSF), or a signal on a brain scan). CSF and blood biomarkers have changed how researchers design trials and how clinicians diagnose AD. Primary tauopathies need similar tools. A reliable blood or CSF biomarker could help families receive better answers faster, help researchers select the right participants for clinical trials, and help companies know whether an experimental treatment is affecting the biology it is meant to change.
Why both tissue and fluids matter
Brain tissue and fluid biospecimens answer different but related questions. Brain tissue is the ground truth; it allows researchers to confirm which disease process was present, where tau accumulated, which cells were affected, and whether other diseases were present at the same time. That tissue is essential for validating any biomarker that claims to identify a specific tauopathy.
Fluids create a different opportunity. Blood, plasma, serum, CSF, and extracellular vesicles can be collected while a person is living. They can sometimes be collected repeatedly, creating a timeline of disease biology. This enables a biomarker to be useful in real life before an autopsy—and ideally early enough to guide care, clinical trial enrollment, and treatment development.
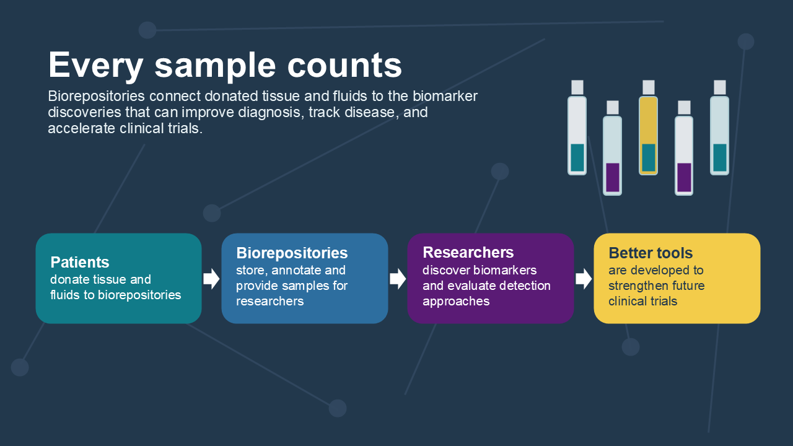
Biorepositories are the bridge between these two worlds. They collect, process, store, annotate, and distribute biological samples. The best repositories do not simply freeze tubes. They link samples to carefully collected information: diagnosis, age at collection, sex, clinical measures, genetic results, imaging, medication exposure, sample volume, processing time, storage conditions, and whether the same donor later had a neuropathological diagnosis. Without those details, a vial of plasma is much less informative. With them, it can become a key piece of evidence.
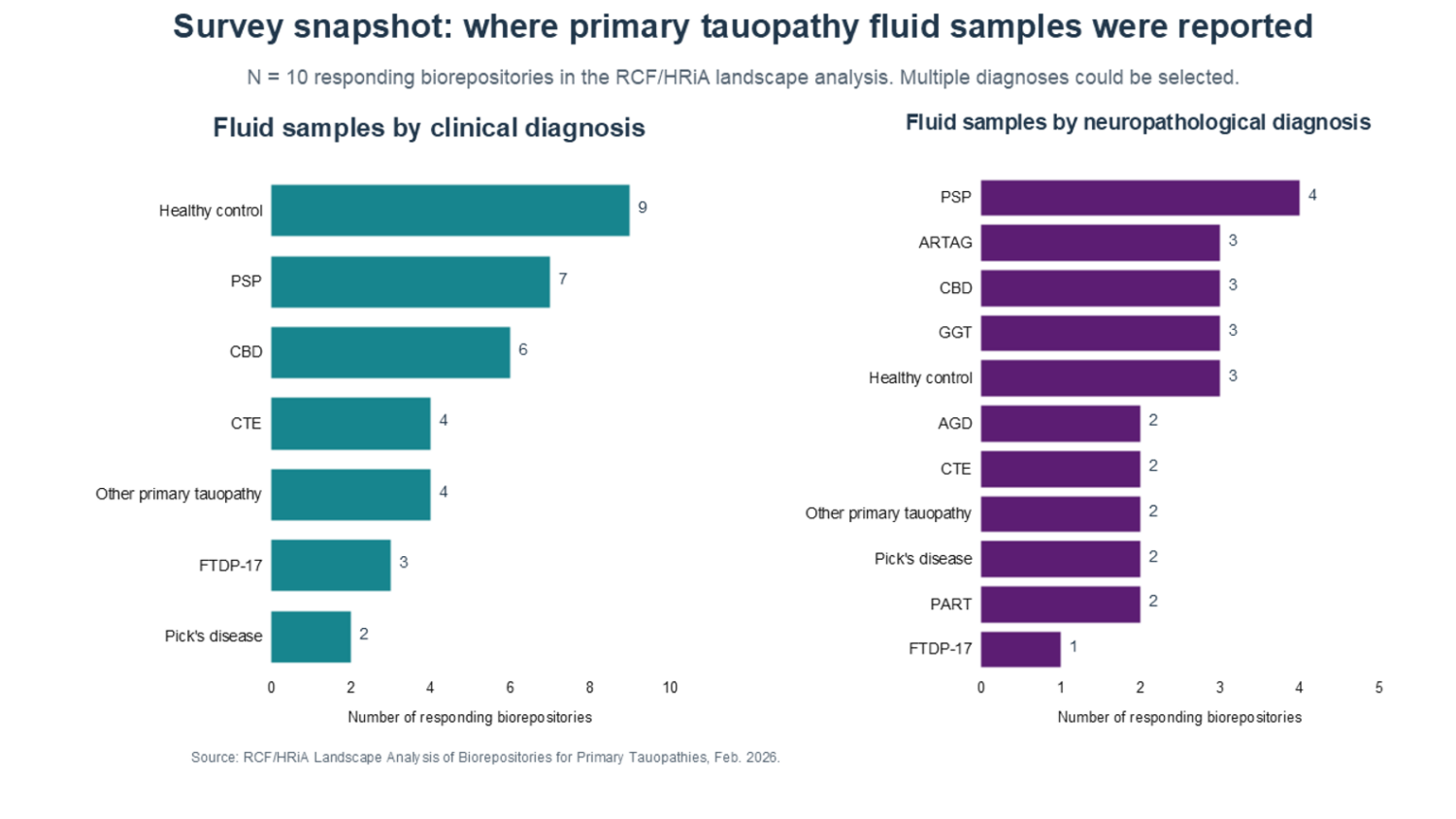
Recently, the Rainwater Charitable Foundation (RCF) partnered with Health Resources in Action (HRiA) to map the biorepository landscape for primary tauopathies. HRiA reviewed the literature and public databases, interviewed stakeholders across academia, industry, biorepositories, and partner organizations, surveyed repositories holding primary tauopathy fluid biospecimens, and developed a searchable Excel-based database. The result is a clearer view of both the opportunity and the bottlenecks.
The sample access journey
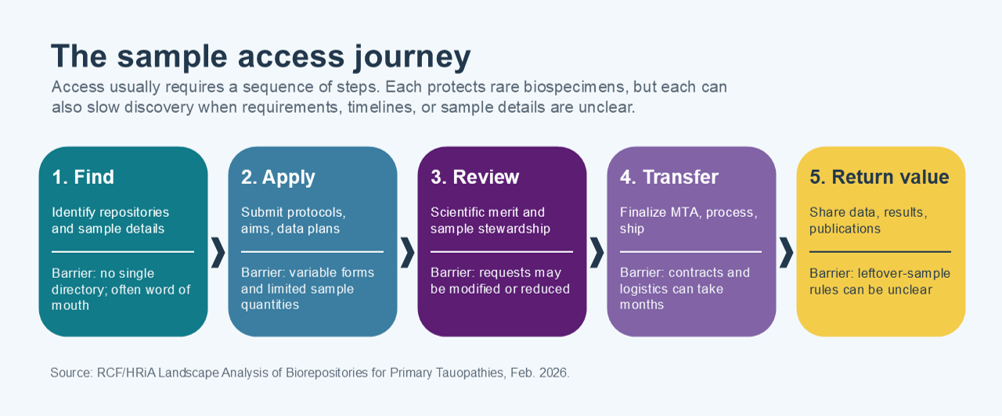
One finding stands out: obtaining samples goes beyond a single transaction—it is a journey. Researchers first must identify which repositories have relevant tissue or fluids. Then they must understand what sample types are available, what diagnoses are represented, whether the samples have associated clinical data, and whether the repository’s consent and governance rules allow the proposed research. Applications may require detailed protocols, preliminary data, data-sharing plans, and institutional approvals. Given the rarity of these samples, requests are reviewed for scientific merit and stewardship. If approved, a material transfer agreement (MTA) must be finalized before samples are processed and shipped. After the project, researchers may be asked to return data or findings to continue improving the repository for the next study.
Although each of those steps has a purpose, they can slow discovery. Researchers described relying on professional networks because there is no single, comprehensive directory of repositories and inventories. Application requirements vary, and sample volumes may be smaller than requested because a repository has to protect limited material for future studies. Collection and storage methods can vary across sites, making results harder to compare. MTAs can take many months and leftover-sample policies can be unclear. For industry partners, data-sharing and commercial-use restrictions can add additional complexity.
The survey snapshot also shows why access matters. Ten responding biorepositories reported samples across a range of diagnoses. Clinical fluid samples were most reported for healthy controls, PSP, and CBD. Fewer samples were available for CTE, FTDP-17, Pick’s disease and other unspecified primary tauopathies. Neuropathologically-linked fluid samples were less common overall, with PSP most frequently reported and several other diagnoses represented by only a few repositories. That is not a failure of the biorepositories but reflects the biology and logistics of studying rare diseases. Every well-annotated sample has high value.
What makes a sample powerful
A useful biospecimen is both biological and informational. A tube of blood becomes far more useful when it is linked to a clear diagnosis, visit date, clinical scales, medications, imaging, genetics, and information about how the tube was handled. For primary tauopathies, one detail is especially important: whether a living clinical diagnosis is later connected to neuropathology. That link allows researchers to test whether a proposed biomarker truly points to PSP, CBD, or another tauopathy rather than to a look-alike syndrome.
This is also where tissue and fluids reinforce each other. Brain tissue can verify the final disease biology. Fluids can show whether that biology left a measurable signal in blood or CSF in a living person. Longitudinal samples can show whether the signal changes as symptoms progress. When repositories can connect these layers, researchers can move from a simple question like, “is this protein higher or lower?” to a more useful one like, “does this marker identify the right disease, at the right time, and in the right person with enough reliability to guide a trial?”
Trust, quality and donor partnership
Better biorepository infrastructure is also a matter of trust. Patients and families donate samples with the hope that their contribution will help others. That trust is strengthened when repositories collect samples responsibly, explain how material may be used, protect privacy, return value to the research community, and make participation possible for more communities. If access depends on who you know, less-established researchers and smaller institutions will be left out. A transparent directory and clear policies can make the system both fairer and faster.
Access is not only about permission but also about quality. Biomarker discovery is especially sensitive to pre-analytical variables. That is, the details of how a sample was collected, processed, aliquoted, frozen, thawed, stored, and shipped. A protein measured in plasma can look different if one site processed blood immediately and another site waited hours, or if one vial has been thawed several times. In multi-site research, standard operating procedures and shared metadata make samples more comparable and results more reproducible.
Public resources show that coordination is possible. The NIH NeuroBioBank centralizes access to post-mortem brain tissue through a network of repositories and distributes thousands of samples per year for research. The RCF’s own tauopathy resources page provides investigators with data, cell lines, and biospecimen resources such as ALLFTD and NCRAD-linked materials. These examples do not solve every primary tauopathy need, but they illustrate the importance of making resources visible, governed, and usable.
A practical agenda for faster biomarker discovery
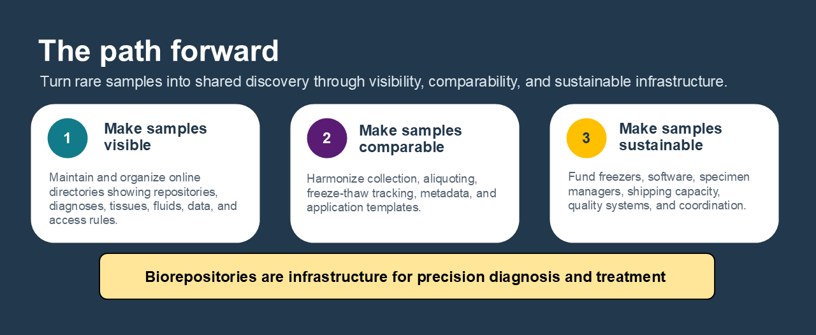
The path forward is not mysterious. First, create and maintain a living directory of primary tauopathy biorepositories that includes diagnoses, sample types, sample quantities or availability ranges, associated data, access rules, expected timelines, contact information, and whether tissue confirmation exists. Second, streamline applications and policies where possible: common request templates, clear review criteria, standard data-return expectations, and transparent guidance for leftover samples. Third, fund the infrastructure that rarely receives enough attention: freezers, inventory software, servers, specimen managers, shipping capacity, quality-control systems, and staff time. Altogether, the aim is to make biorepository stewardship more useful and transparent.
For families affected by primary tauopathies, a donated sample is an act of trust. For researchers, it is a chance to ask a question that could not be answered any other way. For funders, it is a reminder that discovery depends on infrastructure as much as ideas. Biorepositories for primary tauopathy tissues and fluids are not background operations—they are the connective tissue of biomarker science. When they are visible, well-funded, standardized, and collaborative, each sample can travel farther, from one donor’s generosity to a future diagnostic test, trial endpoint, or therapy.
To learn more, download our recent report.